Provider Alignment in Rural Markets and Micropolitan Markets
This sponsor content is part of AHLA's 2026 Health Care Transactions Resource Guide
- March 24, 2026
- Curtis Bernstein , Pinnacle Healthcare Consulting
- Peter Kim , Pinnacle Healthcare Consulting
Two goals of the Rural Health Transformation Program are to strengthen workforce pipelines and support innovative care delivery models. Those objectives are easy to articulate but difficult to execute in rural and micropolitan markets, where low patient volumes, challenging payer mix, geographic isolation, and limited physician supply can make traditional recruitment and compensation strategies difficult to sustain. Even so, physician compensation arrangements can still be structured to support access, care coordination, and quality improvement--provided they are commercially reasonable, consistent with fair market value, and tied to identifiable services and measurable performance objectives.[1]
What is a Rural or Micropolitan Market?
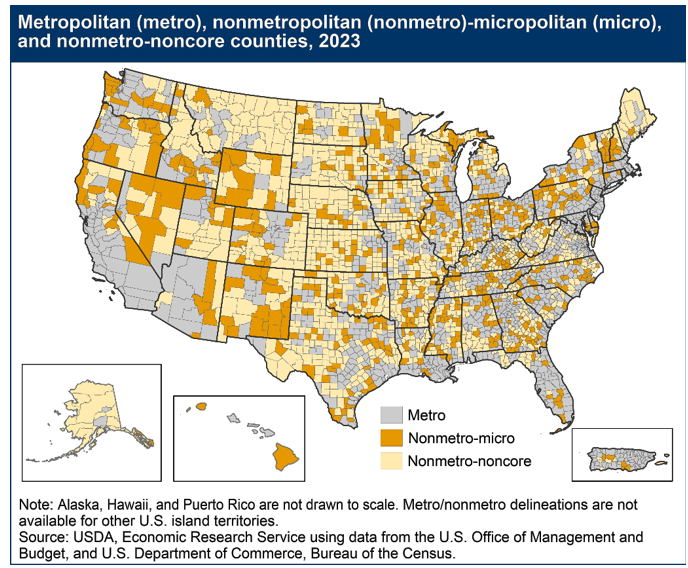
There is no single universal federal definition of “rural,” and different agencies use different classification frameworks. In practical terms, however, rural and micropolitan markets generally share several characteristics relevant to physician alignment: smaller populations, lower provider density, greater travel distances, and less scale than metropolitan markets. Some communities are truly rural, while others are micropolitan--nonmetropolitan areas organized around a smaller urban core. That distinction matters because small towns adjacent to metropolitan areas may face different labor, referral, and access dynamics than communities that are both smaller and more geographically isolated. Currently, 64% of all non-metro areas are rural while 12.9% of all metro areas are rural.[2],[3] The Phase III Final Stark Rules defines a micropolitan area as “a single urbanized core population of at least 10,000 but less than 50,000 population.”[4]
How Limited is Supply of Providers in these Markets?
Nonmetropolitan communities still represent a meaningful share of the U.S. population, making provider shortages in these markets a significant access problem rather than a fringe issue. USDA reports that nonmetro counties account for about 14% of the U.S. population, or just over 46 million people.[5] Federal research also shows that rural communities generally face lower incomes, more insurance and access barriers, older populations, and greater care-delivery challenges than urban markets. On average, households in these markets have 7% lower incomes than urban areas and are 1.7% less likely to be insured. Further, rural markets are getting older with 4% more of the population over 65 years old and the percent of the population increasing annually. The aging population creates unique issues related to mobility, especially as it relates to the distances traveled to get healthcare, and when combined with the lacking infrastructure of rural markets to seek care (inability to drive, discomfort of driving in a metro area, or simply lack of transportation).
These communities also tend to present greater disease burden and less favorable health indicators, including worse morbidity indicators and patients with more co-morbidity as well as:
- Higher rates of maternal and infant morbidity;
- More death from heart disease, cancer, and stroke;
- Higher mental and behavioral health issues; and
- Higher rates of cigarette smoking and lower rates of exercise.[6]
Rural residents also face non-financial barriers to care, including transportation limitations and longer travel distances to obtain services.
The delivery infrastructure supporting these markets is also under strain. The number of hospitals supporting providers in these markets has been declining for decades. The UNC Sheps Center reports 195 rural hospital closures and conversions since January 2005, including 152 since 2010. At the same time, rural obstetric access continues to decline; by 2022, only 41.2% of rural counties had hospital-based obstetric services.[7] In 2023, CMS created the Rural Emergency Hospital provider type to help preserve emergency and outpatient access in communities where maintaining inpatient services is no longer feasible.[8]
Workforce projections suggest that provider shortages in these communities will remain a long-term issue. The Commonwealth Fund reports that by 2037, the current supply of rural primary care physicians is expected to meet only 68% of demand, and that 43 million people live in rural areas with primary care health professional shortages. The same report found that only 19% of rural adults received primary care via telehealth, compared with 29% nationally. Federal workforce programs such as the National Health Service Corps also continue to support recruitment by offering loan repayment and scholarship opportunities for clinicians serving in Health Professional Shortage Areas.[9]
What Can Entities in These Markets Do to Recruit and Align with Providers?
When aligning with physicians, regulatory compliance is a central consideration. Rural status may affect how certain rules apply, but it does not eliminate the need to analyze Stark Law, Anti-Kickback Statute, fair market value, and commercial reasonableness requirements.
Even in rural or micropolitan settings, compensation arrangements involving designated health services must satisfy an applicable Stark Law exception and should be structured with clear attention to compliance fundamentals.[10] Under the Stark Law, an agreement must be:
- For identifiable services;
- Set at a compensation level that is fair market value for the services and not paid based on the value or volume of referrals; and
- Commercially reasonable (i.e., the parties would have entered into the arrangement even if one entity was not referring patients to the other party).
Providers may engage through employment agreements, independent contractor agreements, professional services agreement or a variety of other types of affiliation agreements.[11]
Health System Strategies and Partnerships
Rural and micropolitan hospitals can join together through a regional collaboration or partner with larger local systems. These partnerships allow the hospital to participate in value-based enterprises and possibly work together to negotiate insurance contracts. At least 40 of these partnerships are already in existence. Some of the partnerships have formed accountable care organizations for their members hospitals.
With limited means in which to measure quality, these partnerships have worked together to measure certain quality indicators and then work together on best practices to improve quality across the region. Certain examples are colorectal or depression screenings.[12]
Non-Physician Workforce Strategies
With the limited amount of physician resources, hospitals will commonly use a team-based approach including advanced practice professionals (APPs), emergency medicine technicians, and non-provider staff. In these markets, APPs provide almost twice the amount of patient visits than they do in urban markets and a lot of time they operate without physician supervision. Multidisciplinary care teams are often the most practical and scalable way to maintain access and continuity in areas where physician supply alone cannot meet demand.[13]
Fully Deployed Telehealth Models
Telehealth services originally were implemented in homes to allow patients to see primary care physicians. Today, telehealth has expanded within the walls of the hospital and outside into schools, long term care facilities, specialty rehabilitation facilities, and other locations. Telehealth provides support to hospitals continuously, which reduces inappropriate admissions and reduces unnecessary transfers (as an example). Certain markets can expand on services such as dialysis, which can also lead to additional patients allowing the facilities to expand into other areas like cardiology.[14]
How is Fair Market Value Determined?
Fair market value in rural and micropolitan markets is not determined simply by selecting a national benchmark percentile and applying it without adjustment. Under the Stark regulations, fair market value means the value in an arm’s-length transaction, consistent with the general market value of the subject transaction, and compensation should reflect bona fide bargaining between well-informed parties not otherwise in a position to generate business for each other.[15] In practice, that means the analysis should consider specialty, service mix, schedule, call obligations, administrative duties, travel burden, local supply constraints, and the commercial realities of the community being served.
Providers in these markets may furnish services through in-person clinics, hospital-based care, episodic onsite coverage, telemedicine, or hybrid models. Compensation should therefore reflect not only personally performed clinical services, but also other legitimate duties that may be necessary to sustain access in the market, such as emergency department call coverage, medical directorship responsibilities, care coordination oversight, or other administrative services. That type of context-specific design is consistent with the broader fair market value and commercial reasonableness framework applied under Stark. The recruitment challenge is often especially acute in core specialties and service lines needed to support local access, including:
- Anesthesiology, including certified registered nurse anesthetists;
- Cardiology;
- Emergency Medicine;
- Gastroenterology
- General Surgery;
- Orthopedic Surgery;
- Pediatrics;
- Primary Care (including APPs);
- Psychiatry; and
- Urology.
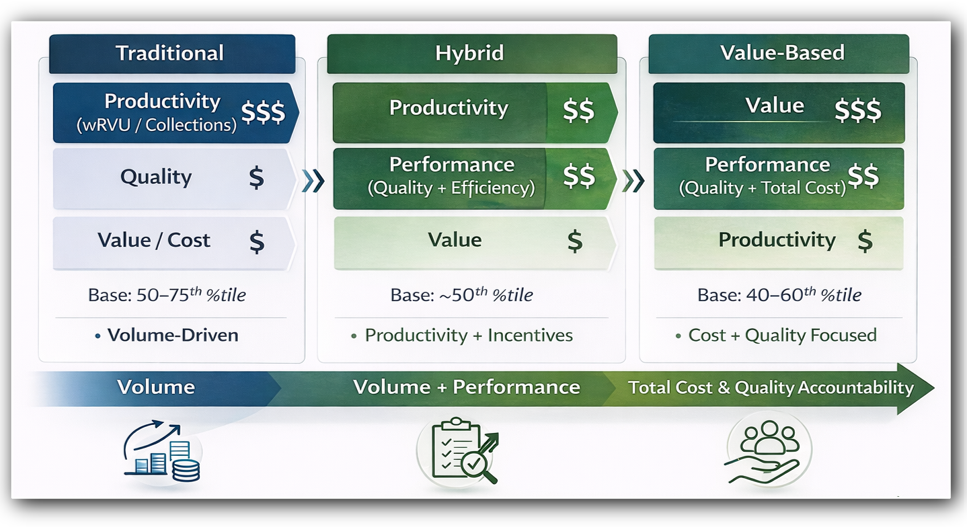
Benchmarking for selected specialties may show that total compensation in rural and micropolitan markets exceeds compensation levels in suburban or urban settings even where productivity, as measured by wRVUs, is not proportionately higher. In a review of compensation data presented in the MGMA DataDive for these specialties in rural and micropolitan markets, the data presented shows about a 25% premium in compensation for about the same amount of work in suburban or urban markets as determined based on wRVUs.[16] The majority of the premium is driven by the subspecialists (e.g., anesthesiology, cardiology, gastroenterology, orthopedic surgery, and urology). While some of these premiums are driven by higher productivity, in practice, that pattern often reflects persistent recruitment and retention difficulty, local scarcity, travel burden, and coverage demands rather than purely higher clinical output.
To better align physician incentives with care delivery goals, some organizations are moving beyond purely volume-based compensation and incorporating objective performance components tied to quality, access, care coordination, or panel management. In practice, these models often combine a base component for personally performed clinical services with carefully defined supplemental components for call coverage, administrative responsibilities, or pre-established performance metrics. Any such model must still be supported by fair market value analysis and structured to avoid rewarding referral volume. CMS’s rural transformation initiatives also reflect a broader policy shift toward delivery models that strengthen access and care coordination in underserved communities.[17]
One practical example is readmissions. CMS describes the Hospital Readmissions Reduction Program as a Medicare value-based purchasing program intended to improve communication, care coordination, and discharge planning to reduce avoidable readmissions.[18] Many rural hospitals, including critical access hospitals and other facilities outside the applicable subsection (d) framework, are not directly subject to the same HRRP payment mechanics. Even so, avoidable readmissions still create meaningful financial and operational strain, which makes care coordination and post-discharge follow-up relevant design considerations in rural physician alignment models.

Of course, identifying potential opportunities through provider affiliation agreements is easier than implementing such programs. Accordingly, provider involvement in the development, implementation, and continued support of such a program is vital. Without physician buy-in, even a well-drafted compensation model may fail in practice. To be durable, the arrangement must be operationally workable, clearly communicated, and responsive to the actual clinical and community needs the parties are trying to address. That is particularly true in rural and micropolitan markets, where successful alignment depends not only on legal compliance and fair market value, but also on sustained provider engagement and a realistic approach to care delivery.
Conclusion
Rural and micropolitan markets present a distinct physician alignment challenge: patient need is substantial, provider supply is constrained, and traditional compensation assumptions often do not fit the economics of the market. Yet these conditions do not prevent alignment; they require more disciplined alignment. Compensation arrangements in these settings should be built around identifiable services, fair market value, and commercial reasonableness, while also recognizing the operational realities of recruitment, call burden, care coordination, and long-term access. When structured thoughtfully, physician alignment models in rural and micropolitan markets can help stabilize care delivery and improve community health outcomes.
[1] Centers for Medicare & Medicaid Services. (2026, March 12). Rural Health Transformation (RHT) Program. U.S. Department of Health and Human Services. https://www.cms.gov/priorities/rural-health-transformation-rht-program/overview
[2] U.S. Department of Agriculture, Economic Research Service. (2026, February 9). Rural classifications: What is rural? https://www.ers.usda.gov/topics/rural-economy-population/rural-classifications/what-is-rural
[3] Metropolitan areas can include both urban and non-urban areas.
[4] Office of Management and Budget. (2000, December 27). Standards for defining metropolitan and micropolitan statistical areas (65 Fed. Reg. 82228). Federal Register. https://www.federalregister.gov/documents/2000/12/27/00-32997/standards-for-defining-metropolitan-and-micropolitan-statistical-areas
[5] U.S. Department of Agriculture, Economic Research Service. (n.d.). Ag and food statistics: Charting the essentials—Rural economy. https://www.ers.usda.gov/data-products/ag-and-food-statistics-charting-the-essentials/rural-economy.
[6] Turrini, G., Thalmayer, A., Meit, M., Kreider, R., & Mandle, L. (2024, October). Rural health: The challenges of care delivery in nonmetropolitan communities [Research report]. Office of the Assistant Secretary for Planning and Evaluation, U.S. Department of Health and Human Services. https://aspe.hhs.gov/sites/default/files/documents/6056484066506a8d4ba3dcd8d9322490/rural-health-rr-30-Oct-24.pdf
[7] North Carolina Rural Health Research Program, Cecil G. Sheps Center for Health Services Research. (n.d.). Rural hospital closures. The University of North Carolina at Chapel Hill. https://www.shepscenter.unc.edu/programs-projects/rural-health/rural-hospital-closures/
[8] Centers for Medicare & Medicaid Services. (2026, March 10). Rural emergency hospitals. U.S. Department of Health and Human Services. https://www.cms.gov/medicare/health-safety-standards/certification-compliance/rural-emergency-hospitals
[9] Nuzum, R., Gunja, M. Z., Moran, M., Rustgi, S. D., FitzGerald, M., Zephyrin, L., & Singh, H. (2025, November). The state of rural primary care in the United States. The Commonwealth Fund. https://www.commonwealthfund.org/publications/issue-briefs/2025/nov/state-rural-primary-care-united-states
[10] Franklin, H. (2020, February 5). Being rural can be Stark-friendly. Health Law Observer. Stevens & Lee. https://www.stevenslee.com/health-law-observer-blog/being-rural-can-be-stark-friendly/
[11] Stanger, K. C. (2015). Stark requirements for physician contracts [PDF]. Holland & Hart LLP. https://www.hollandhart.com/pdf/Stark-Requirements-for-Physician-Contracts.pdf
[12] Hostetter, M. & Klein, S. (2023, May). How Regional Partnerships Bolster Rural Hospitals. The Commonwealth Fund. https://www.commonwealthfund.org/publications/2023/may/how-regional-partnerships-bolster-rural-hospitals
[13] Neprash, PhD, H. (2020, March). Team-Based Primary Care in Rural Markets.
[14] Butzner, M. & Cuffee, Y. (2021, August) Telehealth Interventions and Outcomes Across Rural Communities in the United States: Narrative Review. Journal of Medical Internet Research. https://pmc.ncbi.nlm.nih.gov/articles/PMC8430850/
[15] 42 C.F.R. § 411.351 (2025)
[16] Medical Group Management Association. (2026). MGMA DataDive provider compensation benchmarking data [Proprietary database]. Reviewed by authors.
[17] Centers for Medicare & Medicaid Services. (2026, March 12). Rural Health Transformation (RHT) Program. U.S. Department of Health and Human Services. https://www.cms.gov/priorities/rural-health-transformation-rht-program/overview
[18] Centers for Medicare & Medicaid Services. (2026, March 16). Hospital Readmissions Reduction Program (HRRP). U.S. Department of Health and Human Services. https://www.cms.gov/medicare/payment/prospective-payment-systems/acute-inpatient-pps/hospital-readmissions-reduction-program-hrrp
