Federal and State Government Responses: How Telehealth Is Being Harnessed to Address the Coronavirus Pandemic
This Bulletin is brought to you by AHLA’s In-House Counsel Practice Group and the Public Health System Affinity Group of the Hospitals and Health Systems Practice Group.
- March 18, 2020
- Harsh P. Parikh , Nixon Peabody
- Alexandra Busto , Nixon Peabody LLP
- Sarah Swank , Nixon Peabody LLP
- Jill H. Gordon , Nixon Peabody LLP , Los Angeles, CA
- Rebecca Simone , Nixon Peabody LLP
As the health care system braces for a surge of COVID-19 patients, state and federal governments are increasingly looking to telehealth for help. During the last few weeks, medical providers across the United States started, revamped, or expanded their virtual care capabilities. Public health experts, including the Centers for Disease Control and Prevention, agree that a wider adoption of telecommunications in patient care will improve hospital capacity by preventing the additional spread of the virus. In the face of a global pandemic, federal legislators, state governors, and regulators around the country are acting in concert to leverage telehealth.
The policy changes include:
- Expansion of reimbursement for telehealth services, including federal waiver of existing Medicare Fee-for-Service (FFS) restrictions that will last for the duration of the national emergency;
- Greater cross-state licensure exemptions during the outbreak to allow health care providers to render services, including telehealth services, across state lines;
- Enforcement flexibility that will allow providers to offer free telehealth services through widely-available smart phone applications, like Skype and FaceTime; and
- Relaxation of certain limitations to online prescribing to drop initial in-person visit requirements under certain circumstances.
These policy changes reflect the recognition at national and local levels that telehealth will be critical in helping to limit further exposure and stop the spread of COVID-19 in health care settings. In addition, the significant opportunities arising for virtual care, which is at the forefront of the fight against coronavirus, may transform telehealth forever.
Federal Government Expands Medicare Coverage for Telehealth During Emergencies
Existing Medicare Fee-For-Service Reimbursement
The lack of Medicare reimbursement for telehealth is a key roadblock to wider adoption. For decades, Medicare reimbursement for telehealth services was limited to certain circumstances. A patient receiving telehealth services was required to be at an “eligible originating site,” meaning that the patient had to be located in a rural area and in a medical facility.1 The patient’s home was not considered an eligible originating site. In other words, telehealth services provided to a patient located at home were not reimbursable by Medicare under this framework.
Medicare expanded reimbursement for telehealth services incrementally over the past few years. For example, it allowed reimbursement for: (1) brief, patient-initiated communications with a health care practitioner known as “Virtual Check-Ins” with existing patients, and (2) non-face-to-face, patient-initiated communications through an online patient portal, known as “E-Visits.” The most recent appropriations bill removed key restrictions imposed upon virtual care to address the COVID-19 national emergency.
Congressional Expansion of Telehealth to Curb Coronavirus
As part of the federal government’s initial response to the growing pandemic, the bipartisan Coronavirus Preparedness and Response Supplemental Appropriations Act of 2020 appropriated $500 million to telehealth reimbursement, opening the door for the Centers for Medicare & Medicaid Services (CMS) to expand telehealth coverage. The new law amended Section 1135 of the Social Security Act by authorizing the Department of Health and Human Services (HHS) to issue waivers that remove traditional limitations for telehealth in an emergency area during an emergency period. Under the statute, the telehealth waiver authority was automatically triggered by the COVID-19 pandemic.
CMS Guidance on “Blanket” Telehealth Waiver Under Section 1135
On March 16, 2020, CMS exercised its newly granted authority under Section 1135 of the Social Security Act (Section 1135 waiver) to expand telehealth services during the COVID-19 emergency. Clinicians can bill immediately for dates of service starting March 6, 2020. The Section 1135 waiver allows for the following:
- Patient’s Home or Another Facility Can Be an Originating Site. First, the “eligible originating site” requirement no longer needs to be satisfied, meaning that telehealth services may be provided to Medicare beneficiaries regardless of patient location—including at the patient’s home or a physician’s office, hospital, nursing home, or rural health clinic. Under the Section 1135 waiver, Medicare beneficiaries will be able to visit with their doctor from their home, without having to go to a health care facility, and can better avoid putting themselves and others at risk.
- Smart Phones. The Medicare program’s prohibition on telephones was removed for the duration of the outbreak. Current Medicare rules do not permit telephones to be used for telehealth services. Now, so long as the telephone has audio and video capabilities used for two-way, real-time interactive communication, it can be utilized during the COVID-19 pandemic.
- Wide Range of Telehealth Services Available. Notably, the legislation applies to telehealth services during this period without regard to the treatment or diagnosis of the patient. Medicare beneficiaries may receive a range of telehealth services, including typical office visits for evaluation/management, mental health counseling, and preventive health screenings.
- New Patients Are Likely Permissible. On the issue of whether providers can be reimbursed for telehealth services provided to a new patient (i.e., through the Emergency Department), CMS is asking providers to ignore the statutory language that limits the waiver to current patients. The statutory language requires that there be a pre-existing relationship with the patient receiving telehealth services. CMS assures providers that it will not conduct audits to verify that such a prior relationship existed for claims submitted during this emergency period.
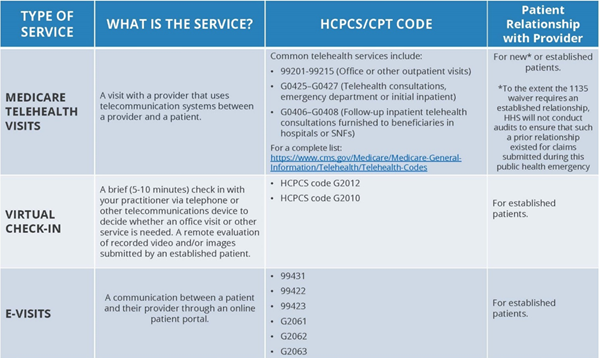
The following table provided by CMS summarizes Medicare FFS reimbursement for telehealth services:
Other Telehealth Reimbursement
Many states continue to restrict Medicaid reimbursement to limited circumstances, but this may also change as telehealth becomes the most viable option for access to care. In efforts to combat the virus, state governors and public health leaders have announced expansions in Medicaid reimbursement in many states. For example, New York has expanded telehealth coverage and reimbursement for disabilities services under Medicaid. It is also important to remember that many state Medicaid managed care plans already authorize telehealth, and some states have already required parity in payment for telehealth. Irrespective of the availability of reimbursement, it is also worth noting that licensure, supervision, and professional judgement are still required, and professional standards of care have not changed.
Loosening of Jurisdictional Licensing Restrictions
Recognizing that the virus does not discriminate by state line, both state and federal regulators are removing licensing barriers for health care providers to care for COVID-19 patients. HHS issued a separate 1135 waiver of the requirement that “physicians or other health care professionals hold licenses in the state in which they provide services if they have an equivalent license from another state.”
State leaders and medical boards are similarly beginning to loosen their restrictions regarding cross-state licensure. For example, New York is permitting unlicensed individuals, upon completion of training deemed adequate by New York’s Commissioner of Health, to collect throat or nasopharyngeal swab specimens from individuals suspected of being infected for purposes of testing. Certain state governors and medical boards are removing home state licensing restrictions altogether. In California, licensure requirements are waived for any out-of-state medical personnel that come to California to provide health care services in an effort to assist in preparation for, respond to, mitigate the effects of, and recover from COVID-19. These efforts are all aimed to increase staffing and the capacity to care for COVID-19 patients.2
Enforcement Discretion to Encourage Telehealth
Given the importance of social distancing and other strategies recommended to reduce the risk of COVID-19 transmission, federal enforcement agencies are giving providers more flexibility, including by allowing providers to offer telehealth services for free and/or making it easy-to-use.
- No Copay/Deductible/Coinsurance Payment for Medicare and Medicaid Beneficiaries. The HHS Office of Inspector General (OIG), the agency that spearheads enforcement of federal fraud and abuse laws, issued a Policy Statement explaining its position that providers may waive cost-sharing obligations (i.e., coinsurance and deductibles) for telehealth services during the emergency period. Routine reductions or waivers of costs by Medicare or Medicaid beneficiaries trigger the federal Anti-Kickback Statute and the Civil Monetary Penalties Law. In addition, CMS, in consultation with the OIG, issued a memo to Medicare Advantage Organizations (MAOs), advising that MAOs may expand telehealth programs and may also routinely waive cost-sharing payments.
- HIPAA Flexibility. HHS Office for Civil Rights (OCR) announced that it will not impose penalties for violations of certain Heath Insurance Portability and Accountability Act (HIPAA) rules, including the lack of a Business Associate Agreement between the provider and the technology vendor, effective on March 17, 2020. OCR confirmed that health care providers may serve patients in good faith through everyday communications technologies, such as FaceTime or Skype, during the COVID-19 nationwide public health emergency without fear of HIPAA enforcement. This flexibility does not apply to the use of public-facing technologies such as Facebook Live, Twitch, or similar video communication apps.
- Drug Enforcement Administration (DEA) Emergency Flexibility: No In-Person Visit for Prescriptions. Health care practitioners that are DEA-registered may issue prescriptions for controlled substances to patients with whom they have not conducted an in-person visit. The prescription must be for a legitimate medical purpose and the telemedicine communication must use live-video.
Conclusion
It appears that federal and state governments and enforcement agencies will continue to find ways to expand much needed access to care during the COVID-19 pandemic. Providers should begin planning their telehealth strategies now to prepare for hospital surges, reduction of physician office visits, or find alternatives to in-office care, such as remote visits. In the fight against the novel coronavirus, providers have more flexibilities and freedom on coverage, modality of technology used, and location of the patient.
Resources
- Answering 20 Questions About COVID-19, Centers for Disease Control and Prevention, March 18, 2020: https://emergency.cdc.gov/epic/learn/2020/webinar_20200318.asp; https://emergency.cdc.gov/epic/pdf/slides_031820_Questions_about_COVID-19.pdf
- Medicare Telehealth Frequently Asked Questions, Centers for Medicare & Medicaid Services, March 17, 2020: https://edit.cms.gov/files/document/medicare-telehealth-frequently-asked-questions-faqs-31720.pdf
- Medicare Telemedicine Health Care Provider Fact Sheet, Centers for Medicare & Medicaid Services, March 17, 2020: https://www.cms.gov/newsroom/fact-sheets/medicare-telemedicine-health-care-provider-fact-sheet
- Executive Order No. 202, Declaring a Disaster Emergency in the State of New York, March 7, 2020: https://www.governor.ny.gov/news/no-202-declaring-disaster-emergency-state-new-york
- Proclamation of a State of Emergency, Executive Department of the State of California, March 4, 2020: https://www.gov.ca.gov/wp-content/uploads/2020/03/3.4.20-Coronavirus-SOE-Proclamation.pdf
- COVID-19 Information Page, U.S. Department of Justice, Drug Enforcement Administration, Diversion Control Unit: https://deadiversion.usdoj.gov/coronavirus.html
- OIG Policy Statement Regarding Physicians and Other Practitioners That Reduce or Waive Amounts Owed by Federal Health Care Program Beneficiaries for Telehealth Services During the 2019 Novel Coronavirus (COVID-19) Outbreak, March 17, 2020: https://oig.hhs.gov/fraud/docs/alertsandbulletins/2020/policy-telehealth-2020.pdf
- Notification Of Enforcement Discretion For Telehealth Remote Communications During The COVID-19 Nationwide Public Health Emergency, U.S. Department Of Health & Human Services, March 17, 2020: https://www.hhs.gov/hipaa/for-professionals/special-topics/emergency-preparedness/notification-enforcement-discretion-telehealth/index.html
1Under these requirements, telehealth services are reimbursable by Medicare only when a beneficiary is at a qualifying “originating site,” meaning a health care facility or doctor’s office in a county located outside of a Metropolitan Statistical Area or that is located in a rural Health Professional Shortage Area, and when provided via an “interactive telecommunications system.” See 42 CFR 410.78(a)(3), (a)(4), (b)(1), (b)(3), (b)(4).
2Note that while interstate coverage requirements of individual clinicians are being loosened, there has been no recognition of the complexity of entities – such as medical practices – performing services across state lines, and there has been no guidance to date or relaxation of requirements for a medical group or other professional entity to do business in another state.